
Prevention Plan
of Action 2.0
2022-2024
The Department’s renewed strategic
approach to prevent self-directed harm
and prohibited abuse or harm
Office of the Under Secretary of Defense
for Personnel and Readiness
May 2022

1
Prevention Plan of Action
Table of Contents
Executive Summary .................................................................................................................. 2
Part 1: Primary Prevention Framework .................................................................................. 3
Part 2. Integrated Primary Prevention .................................................................................. 11
Appendix A .............................................................................................................................. 24
Figure 1. Primary Prevention System ........................................................................................ 5
Figure 2. Primary Prevention Process ....................................................................................... 5
Figure 3. Types of Prevention Activities .................................................................................... 7
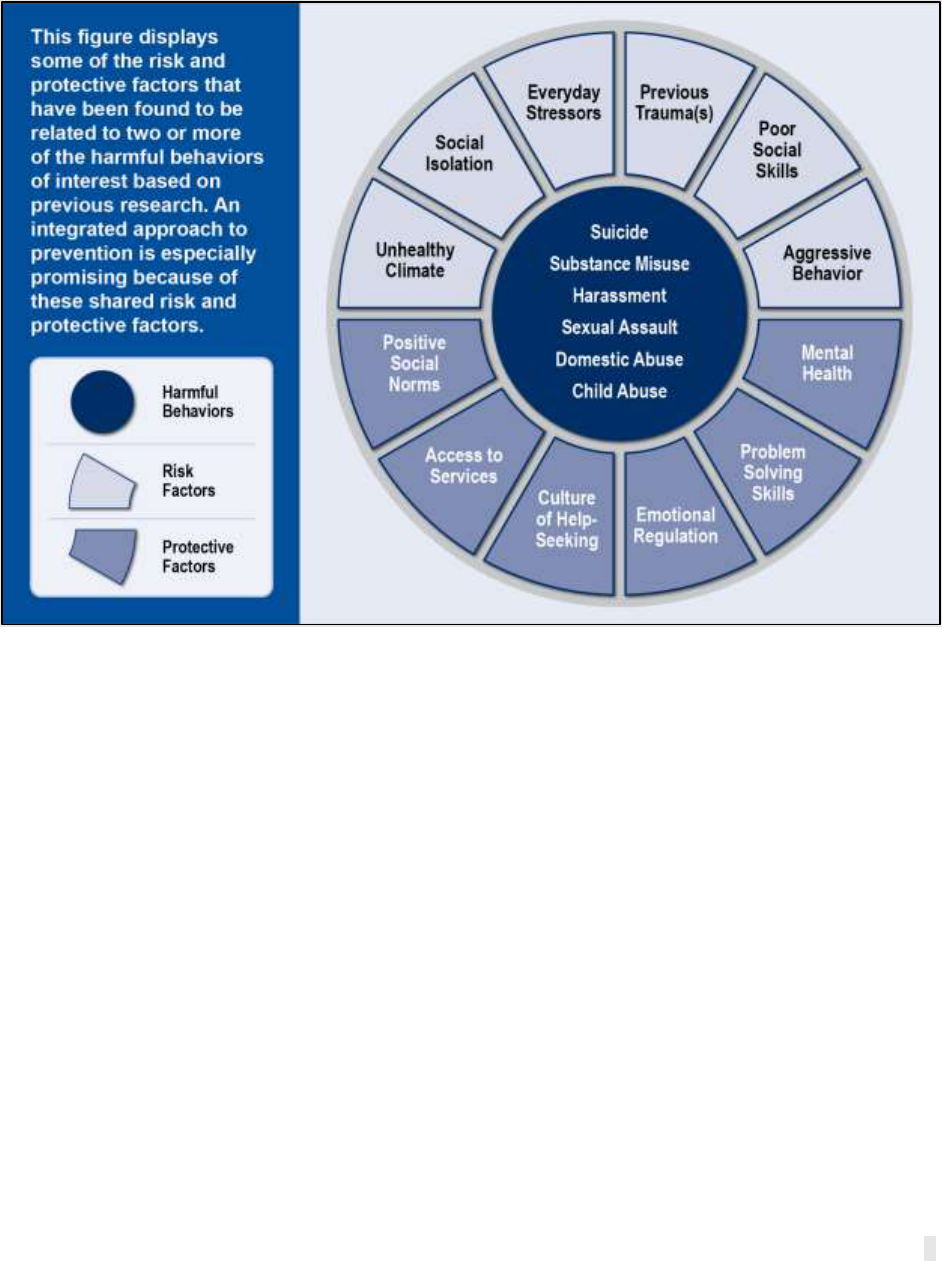
Figure 4. Shared Risk and Protective Factors for Harmful Behaviors ........................................ 8
Figure 5. Evolution of Primary Prevention ................................................................................12

2
Prevention Plan of Action
Executive Summary
Self-directed harm and prohibited abuse or harm refers to sexual assault, harassment,
retaliation, suicide, domestic abuse, and child abuse. These behaviors impact force readiness,
disrupt mission effectiveness, tax scarce resources, and take a human toll. Reduction of these
behaviors demands additional steps to solidify the conditions that will sustain lasting progress,
align efforts to proven approaches, and drive the changes required to achieve the Department’s
vision of a military free from abuse and harm.
This document highlights the Department’s new emphasis on integrated primary prevention.
Integrated prevention will require finding shared solutions to the problems of sexual assault,
harassment, retaliation, domestic abuse, suicide, and child abuse. While this range of harmful
behaviors has diverse and unique prevention needs, these harmful behaviors also share many
risk and protective factors. The Department will synergize existing prevention activities by
strengthening efforts that address these shared factors. This approach will align competing
priorities, increase program effectiveness, ensure efficient use of resources, and help leaders
cultivate safe and healthy climates across the military community.
This revised Prevention Plan of Action (PPoA 2.0) establishes a framework to guide the
development, implementation, and evaluation of integrated primary prevention. Importantly,
PPoA 2.0 builds on past work by reinforcing the tenets outlined in the 2019-2023 Department of
Defense Sexual Assault Prevention Plan of Action (PPoA 1.0). The updated PPoA 2.0
incorporates multiple advancements that have occurred since 2019. Specifically, PPoA 2.0
reflects improvements made during the implementation of PPoA 1.0, incorporates the
requirements and aligns language with DoDI 6400.09, “DoD Policy on Integrated Primary
Prevention of Self-Directed Harm and Prohibited Abuse or Harm,” issued September 11, 2020,
and addresses the approved prevention-related recommendations of the Independent Review
Commission on Sexual Assault in the Military report released on July 2, 2021. In short, this
update expands the scope of the initial PPoA from sexual assault to the integrated prevention of
multiple harmful behaviors, removes completed 2019-2023 PPoA objectives, and aligns
remaining objectives with the IRC recommendations as approved by the Secretary of Defense,
and Congressional requirements.
PPoA 2.0 reflects the Department’s urgent need for integrated primary prevention. However,
many of the harmful behaviors addressed in this document have unique prevention
requirements. Subsequent versions of the PPoA will include these unique requirements and
ensure that the military remains on the cutting edge of prevention science.

3
Prevention Plan of Action
Part 1: Primary Prevention Framework
Introduction
The Department remains dedicated to stopping incidents of self-directed harm and prohibited
abuse and harm before they occur.
1
Since the release of the first Prevention Plan of Action
(PPoA 1.0) in 2019, important developments both within and outside of the military highlight the
Department’s need to evolve and strengthen its prevention strategy over time. In 2020, the
Department published its first integrated primary prevention policy, DoD Instruction (DoDI)
6400.09 “DoD Policy on Integrated Primary Prevention of Self-Directed Harm and Prohibited
Abuse or Harm”, spanning the prevention of sexual assault, suicide, harassment,
2
,
3
domestic
abuse, and child abuse (hereafter referred to as “harmful behaviors”). In 2021, Secretary of
Defense Lloyd J. Austin III called for an Independent Review Commission (IRC) on Sexual
Assault. The IRC made key recommendations to promote healthy climates and prevent multiple
forms of harmful behavior. Recommendation 2.8 of the IRC Report requires the Department to
revise PPoA 1.0 to align with the IRC’s vision for integrated primary prevention in the military.
4
This document reflects the Department’s updated and revised Prevention Plan of Action (PPoA
2.0). The PPoA 2.0 incorporates all relevant guidance, addresses the approved IRC integrated
primary prevention recommendations, new Congressional requirements, and the various forms
of harmful behavior encompassed within DoDI 6400.09. This integrated primary prevention
strategy will accelerate the Department’s prevention efforts while enabling leaders to bolster
shared protective factors and reduce risk factors for the entire military community.
DoD Primary Prevention Framework
Overview
Prevention science has evolved considerably over the past thirty years. Researchers have
discovered new and effective ways to reduce harmful behaviors within communities and
organizations.
5
,
6
While primary prevention is complex, the steps required to diminish prevalence
of harmful behaviors and sustain progress are relatively similar to common planning and
1
The terms “self-directed harm and prohibited abuse or harm” and “harmful behaviors” are used throughout this
document and align with DoDI 6400.09.
2
As defined in DoDI 1020.03.
3
As defined in DoDI 1020.04.
4
As defined in DoDI 6400.09.
5
Basile, K.C., DeGue, S., Jones, K., Freire, K., Dills, J., Smith, S.G., Raiford, J.L. (2016). STOP SV: A Technical
Package to Prevent Sexual Violence. Atlanta, GA: National Center for Injury Prevention and Control, Centers for
Disease Control and Prevention. https://www.cdc.gov/violenceprevention/pdf/sv-prevention-technical-package.pdf
6
National Center for Injury Prevention and Control (U.S.). Division of Violence Prevention. (2017). Preventing
Suicide: A Technical Package of Policy, Programs, and Practices. 62.
https://www.cdc.gov/violenceprevention/pdf/suicidetechnicalpackage.pdf
BLUF: The PPoA is a strategy document intended to orient DoD components to DoD’s integrated
prevention approach and priorities. Senior leaders should use this document as a guiding framework to
ensure their prevention efforts remained aligned with DoD.

4
Prevention Plan of Action
coordination processes used routinely throughout the U.S. Armed Forces.
7
First, primary
prevention requires a holistic, comprehensive approach driven with unity of effort toward the
desired end state. Building this approach requires understanding the current environment,
determining the scope of the local problem, and assessing the organizational factors that enable
prevention. Second, a comprehensive approach is comprised of integrated, research-based
prevention activities,
8
which achieve unity of effort only when implemented as designed in a
conducive, supportive environment. Third, prevention activities require the systematic use of
data-driven tactics to achieve the desired outcomes. Finally, preventing harmful behaviors
requires evaluating change indicators over time, assessing organizational factors to inform
adjustments to the prevention approach, and measuring the effectiveness of specific activities.
9
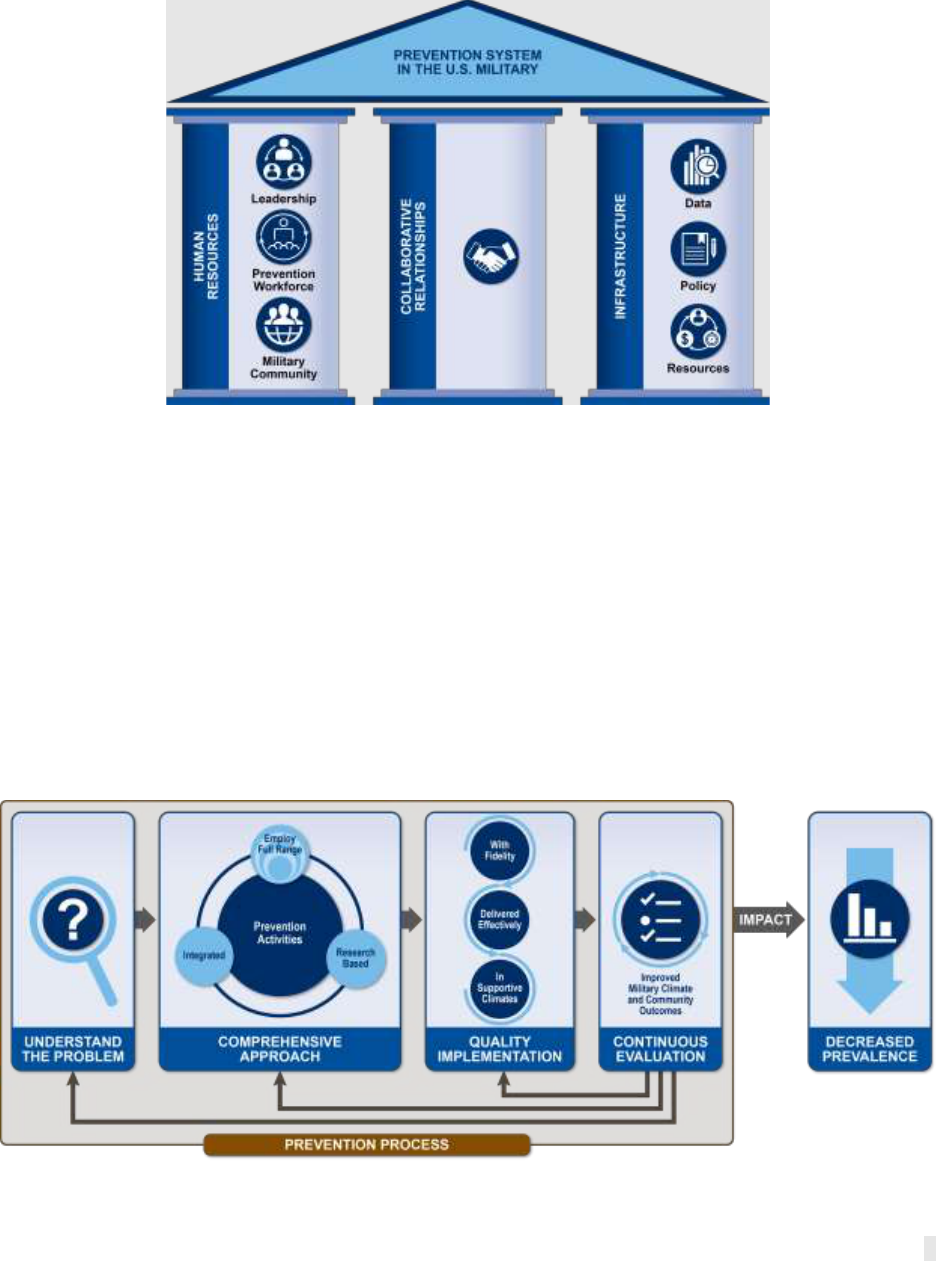
Prevention System Elements
Reducing harmful behaviors across the military community involves enacting the prevention
process in an optimized prevention system (see Figure 1). Organizational factors that constitute
the prevention system include human resources, such as equipped and empowered
leadership, prevention workforce, and the military community; infrastructure, such as
prevention-specific policy, resources, and data systems; and, collaborative relationships
within and across organizations.
10
In an optimized prevention system, human resources
attain and sustain prevention-specific knowledge and skills, collaborative relationships form and
become more productive, and infrastructure facilitates effective planning, implementation,
evaluation, and quality improvement. Too often, prevention activities fail to have an impact
because they are implemented without sufficient development of these system elements. The
policy requirements for implementing the Prevention System are found in DoDI 6400.09 Section
3.1.
7
DoD, Joint Chiefs of Staff, Joint Planning, Joint Publication 5-0 (Washington, DC, 2020).
https://www.jcs.mil/Portals/36/Documents/Doctrine/pubs/jp5_0.pdf?ver=ztDG06paGvpQRrLxThNZUw%3d%3d
8
Research-based policies, programs, and practices are defined as prevention activities selected based on research
evidence that they have shown promise in evaluations to decrease the behavior of interest for a specific population or
that the activity affected one or more contributing factors to the behavior of interest in settings similar to those being
considered for the activity and that positive effects were sustained over time.
9
Basile, K.C., DeGue, S., Jones, K., Freire, K., Dills, J., Smith, S.G., Raiford, J.L. (2016). STOP SV: A Technical
Package to Prevent Sexual Violence. Atlanta, GA: National Center for Injury Prevention and Control, Centers for
Disease Control and Prevention. https://www.cdc.gov/violenceprevention/pdf/sv-prevention-technical-package.pdf
10
Pan American Health Organization. (2014). Plan of Action for the Prevention and Control of Noncommunicable
Diseases in the Americas, 2013-2019. Washington, D.C.: World Health Organization.
https://iris.paho.org/handle/10665.2/35009
5
Prevention Plan of Action
Figure 1. Primary Prevention System
The prevention system is the backdrop against which prevention planning, implementation, and
evaluation all take place. A gap or deficiency in any element of the prevention system (e.g., an
unskilled or underqualified prevention workforce) will degrade the quality of prevention activities.
Prevention Process Elements
The prevention process is a data-driven effort involving four main steps: understanding the
problem, developing a comprehensive approach, quality implementation, and continuous
evaluation. Requirements for the prevention process are outlined in DoDI 6400.09 Section 3.2
and are referred to as “data-driven actions” in the policy. The first step in the primary prevention
process involves understanding the nature and magnitude of a problem within an organization.
This is typically achieved through public health surveillance methods that systematically track
and periodically assess the prevalence (number of people impacted) and incidence (frequency
of occurrence) of a problem over time.
Figure 2. Primary Prevention Process

6
Prevention Plan of Action
The Department has several information collection efforts that assess sexual assault,
harassment, suicide incidents, and related behaviors (e.g., the Workplace Gender Relation
Surveys, DoD Suicide Event Report system). DoDEA Administrative Instruction (AI) 1356.01,
issued in 2018, has helped advance the tracking of child abuse in DoD schools.
11
However, in
the National Guard and Reserves, certain information collection efforts are challenging due to
the part-time nature of the Force and other varied restrictions caused when NG members are
not in a federal status. Furthermore, the Department does not currently have methods to fully
assess the prevalence of domestic abuse and child abuse outside of DoD schools, although
current efforts are underway to generate more information on these harmful behaviors.
After defining the magnitude of the problem, researchers should identify factors known to
contribute to harmful behaviors and their prevention. Generally speaking, contributing
factors are either risk or protective factors. Risk factors increase the likelihood that harm or
abuse will occur. Examples of individual risk factors include previous trauma, substance
misuse, and/or other risky or harmful behaviors (e.g., aggressive interpersonal behavior).
Examples of community-level risk factors include hazing, bullying, retaliation, or other forms of
harassment in the workplace, high drug and alcohol availability, high levels of poverty, and easy
access to lethal means. As such, in a military environment, the Department’s approach to the
prevention of these behaviors is done through a risk-management framework. Protective
factors decrease the likelihood that harmful behaviors will occur. Protective factors also buffer
someone with risk factors from being affected by harmful behaviors. Examples of individual
protective factors include effective communication skills, high levels of social support, and
healthy methods of coping with stress. Examples of community-level protective factors include
an inclusive culture and climate, high cohesion and social connectedness, and social norms that
encourage help-seeking.
12
Risk and protective factors vary substantially depending on the local context, and further vary at
the individual, interpersonal, and community levels. Given the variability of these factors across
the spectrum of harmful behaviors, each organization must conduct needs assessments to
determine which contributing factors should be prioritized for prevention. Combined, the
analysis and dissemination of prevalence survey results, climate assessments, research on
contributing factors, and local needs assessments will provide leaders with the information
needed to guide prevention decision making.
11
AI 1356.01 requires all reports of suspected or alleged incidents of child abuse and neglect to be documented and
reported in a Child Abuse Report (CAR) and reported by phone to the local Family Advocacy Program and Child
Welfare Services within 24 hours.
12
For additional examples of risk and protective factors, see page 14 of the IRC Prevention Appendix.
7
Prevention Plan of Action
Next, after understanding the problem, effective prevention involves developing a
comprehensive approach or plan by applying multiple, reinforcing prevention activities (Figure
3) in a coordinated way to address individual, interpersonal, and organizational factors that
contribute to harmful behaviors. The comprehensive approach should foster healthy
environments and peer norms in addition to building critical personal and interpersonal skills.
For example, alcohol misuse is a risk factor
for sexual assault, suicide, child abuse, and
domestic abuse. However, implementing
policies designed to prevent
overconsumption of alcohol in isolation will
not be sufficient to reduce these harmful
behaviors. Instead, pairing alcohol reduction
policies with prevention education and skill
building programs will reinforce both
prevention activities and may lead to fewer
incidents of harm.
13
In short, the public
health approach examines the environment
and the culture in which individuals live and
seeks to fundamentally change the local
community in ways that stop harmful
behavior before it begins.
Comprehensive approaches ideally combine universal and targeted prevention activities.
Universal prevention activities are activities that engage all Service members, such as building
positive peer environments and promoting shared protective factors. Targeted activities
address the unique needs of high-risk subpopulations. Within large organizations, specific
subpopulations are at higher risk of different forms of abuse and harm. For example, current
data show that young white men are most at risk of dying by suicide in the military, while
women, racial/ethnic minorities, and sexual minority individuals are most at risk of sexual
harassment, and sexual assault.
14
,
15
Pairing targeted prevention activities (i.e., those that
target high-risk groups) with universal prevention activities creates a more robust and efficient
comprehensive approach.
Integrating prevention activities into a cohesive, cross-functional, and cross-organizational
approach yields other advantages, such as promoting unity of effort, avoiding duplication, and
lessening training fatigue. Given the associations among harmful behaviors, a comprehensive
approach for prevention requires the inclusion of activities that effectively boost the cross-cutting
protective factors and mitigate risk factors across the various forms of abuse and harm.
13
Basile, K.C., DeGue, S., Jones, K., Freire, K., Dills, J., Smith, S.G., & Raiford, J.L. (2016). STOP SV: A Technical
Package to Prevent Sexual Violence. Atlanta, GA: National Center for Injury Prevention and Control, Centers for
Disease Control and Prevention. https://www.cdc.gov/violenceprevention/pdf/sv-prevention-technical-package.pdf
14
DoD CY 2020 Annual Suicide Report. Defense Suicide Prevention Office (2021).
2020https://www.dspo.mil/Portals/113/Documents/CY20%20Suicide%20Report/CY%202020%20Annual%20Suicide
%20Report.pdf?ver=0OwlvDd-PJuA-igow5fBFA%3d%3d
15
Trump-Steele, R., Daniel, S, DeMarco, T., Sampath, S., Severance, L., Klahr, A. (2021). Experiences of sexual
minority active duty service members with sexual harassment and sexual assault: Analysis of the 2016 and 2018
WGRA. (Report No. 2021-23). Alexandria, VA: Office of People Analytics.
• Policy: A course or principle of action of a
government or other institution that may be
reflected in regulation, procedure,
administrative action, incentive, or voluntary
practice
• Program: Curriculum or manualized set of
activities and information intended for
learning and skill development
• Practice: Discrete behavior or action
contributing to prevention
Figure 3. Types of Prevention Activities
8
Prevention Plan of Action
The specific prevention activities that address individual, interpersonal, and organizational risk
and protective factors must be complementary, such that messaging, or skills are mutually
reinforcing rather than eroding. Selecting multiple activities that employ a similar approach—
such as building skills for bystanders to intervene in high risk situations—are not sufficient to
ensure compatibility, since different bystander intervention programs may have conflicting
branding and messaging. Instead, various domains of the community must be targeted
simultaneously. For example, building crucial skills and abilities for young adults such as
financial decision-making and effective communication habits can help protect young adults
from domestic abuse and suicide. Increasing connectivity and developing strong support
networks for individuals at risk of isolation can decrease the likelihood of sexual assault
victimization, sexual harassment, and suicide. Maintaining clean, safe housing and providing
affordable, accessible childcare can reduce the risk of child abuse.
Prevention policies, programs, and practices in a comprehensive approach must be selected
because of their evidence base and likelihood to impact harmful behaviors or change the factors
contributing to harmful behaviors. Research-based prevention activities are efforts that have
been rigorously evaluated and shown to decrease specific forms of abuse and harm for a
specific population. Ultimately, implementation of research-based prevention provides the
greatest confidence that prevention activities will decrease harmful behaviors.
Figure 4. Shared Risk and Protective Factors for Harmful Behaviors
9
Prevention Plan of Action
Although implementation of a research-based prevention activity is a significant undertaking and
critical step to decrease prevalence, the quality of implementation is equally important.
16
The
manner and context in which prevention activities take place have a direct effect on the potential
success of a comprehensive approach. Leaders and prevention personnel must implement
prevention activities with fidelity in supportive climates. Fidelity refers to the degree to which
an activity is implemented competently and as designed. While adaptation of activities is
sometimes necessary to appeal to different participants, the key effective ingredients of the
activity must be retained. For example, shortening a prevention program from its original,
validated duration or delivering it with unprepared facilitators can alter its efficacy. A supportive
climate includes leadership buy-in, organizational motivation to implement an activity, and/or
staff with specific skills to implement the activity. Attempting to implement prevention activities
in an unsupportive climate decreases their potential impact.
Once a comprehensive approach is implemented in a supportive climate, it must be
continuously evaluated to determine if its component activities are changing the factors they
were designed to address. This includes evaluation of activities and program outputs (e.g.,
number of leaders trained, number of meetings held with external stakeholders) as well as
evaluation of program outcomes, such as lower rates of harassment. Outcome evaluation
identifies if and to what extent an activity actually decreased negative behaviors and increased
healthy behaviors. Ongoing evaluation is critical for continuous quality improvement.
Documenting challenges and success is also important as the Department continues to build a
repository of best practices. Prevention personnel will learn which prevention activities work
with different populations over time, adjusting implementation when necessary to increase
effectiveness.
Before the prevention process can be fully successful (Figure 2Error! Reference source not
found.), each of the prevention system elements (Figure 1) must be in place. For example,
implementing a prevention activity requires personnel time and training. In the absence of a
prevention workforce, other personnel may be dual-hatted to implement the prevention activity,
which can overtax a military organization leading to decreases in leader buy-in. Lack of buy-in
related to overtaxing the organization may be perceived by subordinate leaders as lack of buy-in
to the activity. Even if the prevention activity had the potential to reduce harm, not attending to
the human resources necessary to implement the activity will decrease effectiveness.
Therefore, there is a symbiotic association between the system elements and prevention
process. Both must be developed and promoted.
16
Wandersman, A., Alia, K., Cook, B.S., Hsu, L.L., and Ramaswamy, R. (2016). Evidence-based Interventions are
Necessary but Not Sufficient for Achieving Outcomes in Each Setting in a Complex World: Empowerment Evaluation,
Getting to Outcomes, and Demonstrating Accountability. American Journal of Evaluation 37, no. 4: 544-561.
https://journals.sagepub.com/doi/full/10.1177/1098214016660613

10
Prevention Plan of Action
To summarize, effective primary prevention involves tackling every step of the prevention
process (Figure 2) within a complete and well-organized prevention system (
Figure 1). The prevention system enables the planning and coordination of prevention and
includes: Human Resources (Leadership, Prevention Workforce, Military Community),
Collaborative Relationships, and Infrastructure (Data, Resources, and Policy). Specific steps in
the prevention process include understanding the problem and contributing factors, developing
a comprehensive approach that targets contributing factors and engages Service members in
solutions, implementing the comprehensive approach with fidelity in supportive climates, and
evaluating the comprehensive approach. The combination of all of these elements is necessary
to decrease the occurrence of harmful behaviors and sustain reductions over time.
Prevention Oversight
The integration and coordination of prevention activities across sectors
17
and settings is
essential for sustaining the impact of primary prevention efforts.
18
Oversight, or efforts to
monitor the degree to which the prevention system and the prevention process are functioning
efficiently and as intended, is the last element of a complete prevention strategy. Oversight will
17
Several important sectors span civilian-military lines and collaboration across sectors—in accordance with law and
DoD regulations—is helpful when implementing large scale prevention strategies. Such sectors include education,
government (local, state, and federal), social services, health services, business/labor, justice, housing, media, and
organizations that comprise the civil society sector such as crisis centers, local health coalitions, faith-based
organizations, youth-serving organizations, foundations, and other non-governmental organizations. Collectively,
these sectors can make a difference in preventing abuse and harm by impacting the various contexts and underlying
risks that contribute to harmful behaviors. See page 33 in Basile, K.C., DeGue, S., Jones, K., Freire, K., Dills, J.,
Smith, S.G., & Raiford, J.L. (2016). STOP SV: A Technical Package to Prevent Sexual Violence. Atlanta, GA:
National Center for Injury Prevention and Control, Centers for Disease Control and Prevention.
https://www.cdc.gov/violenceprevention/pdf/sv-prevention-technical-package.pdf
18
Stone, D., Holland, K., Bartholow, B., Crosby, A., Davis, S., & Wilkins, N. (2017). Preventing Suicide: A Technical
Package of Policy, Programs, and Practices. Atlanta, GA: National Center for Injury Prevention and Control, Centers
for Disease Control and Prevention. Preventing Suicide: A Technical Package of Policy, Programs, and Practices.

11
Prevention Plan of Action
involve monitoring and evaluation of each element of the prevention system (see
Figure 1): including setting knowledge standards for the prevention workforce, military
community, and military leaders, ensuring collaborative relationship are sustained over time,
and tracking prevention data, resources, and policies. For prevention programs, policies, and
practices, oversight will involve establishing and tracking measures of performance and
measures of effectiveness associated with each step of the prevention process (i.e., identifying
the problem, developing a comprehensive approach, implementation, and evaluation). In large
organizations, oversight becomes critical to ultimately achieving long-term prevention goals.
Successful oversight will prioritize outcomes, guide diverse stakeholders, avoid duplication,
ensure consistent messaging, and hold organizations and offices accountable for their progress.
Part 2. Integrated Primary Prevention
History of Integrated Primary Prevention within DoD
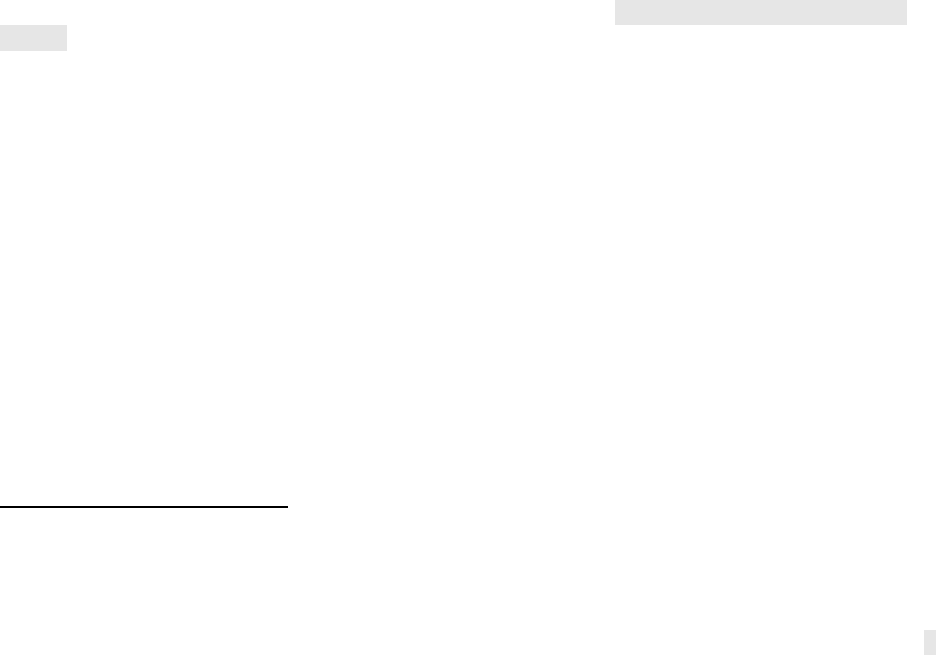
The Department’s approach to primary prevention has evolved over time. As depicted in Error!
Reference source not found., the Department adopted a public health approach to prevention
because methods used to stop and reduce diseases can be adapted and used to prevent
harmful behavior. The offices leading this work initially focused much of their effort
implementing prevention activities proven to reduce harm in the civilian sector and evaluating
ongoing activities that did not yet have an evidence base of effectiveness. Through this phase
of prevention, the importance of quality implementation became clear, such that an effective
prevention activity that was not implemented as intended did not have the intended impact. As
such, the Department’s approach evolved to address both what was implemented (evidence-
based practice) and how it was implemented (with quality).
12
Prevention Plan of Action
Figure 5. Evolution of Primary Prevention
As prevention policies and practices evolved, the Department’s data began to show that climate
factors such as toxic leadership, harassment (including hazing and bullying), discrimination, and
lack of social support increased the risk for multiple harmful behaviors. At the same time, data
began to accumulate suggesting Service members and DoD civilian personnel found training
and education across harmful behaviors to be duplicative: often addressing the same risk or
protective factors.
19
As a result, leadership across DoD sought to identify opportunities to
synchronize prevention activities by leveraging shared risk and protective factors that contribute
to multiple harmful behaviors.
Rather than simply combining or sequencing prevention activities to reduce redundancy,
integrated primary prevention involves taking action to decrease harmful behaviors and
reduce their impact on readiness and retention in a way that:
• Incorporates values of inclusivity, connectedness, dignity and respect (access, equity,
rights, and participation)—including the elevation of Service member and family member
voice—to inform plans, processes, and trainings;
• Recognizes and adjusts plans, processes, and trainings to consider and be responsive
to climate issues and populations that have been disproportionately impacted by harmful
acts;
2018 Workplace and Gender Relations Survey of Active Duty Members: Overview Report. Report No. 2019-027.
Alexandria, VA: Office of People Analytics, 67-68. https://apps.dtic.mil/sti/citations/AD1072334

13
Prevention Plan of Action
• Intentionally seeks to align and find common operating principles across prevention
efforts and offices (e.g., equal opportunity, drug reduction response, suicide prevention,
sexual assault prevention); and,
• Incorporates multiple lines of effort across individual, interpersonal, and
community/organizational levels.
20
Integrated primary prevention addresses shared risk and protective factors across harmful
behaviors through integrated solutions, while maintaining prevention activities that may be
unique to a specific harmful behavior.
In addition to the factors outlined in Figure 4, pre-military experiences and conditions must be
considered when implementing integrated primary prevention activities. The social
determinants of health are the circumstances in which people are born, grow, work, live, age,
and the wider set of forces and systems shaping the conditions of daily life. The fact that certain
groups and communities are disproportionately impacted by abuse and harm is not a
coincidence. In some cases, the increased risk for exposure to harmful behaviors and
associated negative health outcomes is a result of longstanding, systemically unjust economic
and social policies. For example, policies still exist today that maintain neighborhoods of
concentrated poverty and limit access to 1) quality schools, 2) health services, and 3) social
support—all factors that protect against harmful behaviors and other adverse health conditions.
Exposure to negative conditions in early childhood
21
is associated with increased risk of poor
health and further adverse experiences at every subsequent life stage, placing some individuals
and groups at greater risk for harmful behaviors during military service.
People join the military with different backgrounds and experiences. Each individual’s
background and experiences affect who they are, the decisions they make, and how they
interact with others. Some individuals bear the burden of past or current hardships based on
race, sexual orientation, religion, or ethnicity and those experiences impact their day-to-day
lives. The DoD has enacted policies—such as housing, childcare subsidies, and equal pay for
equal work—to create equal opportunities; however, equal opportunity is not necessarily
enough to ensure equity due to past hardships based on racism, sexism, homophobia, and
other types of discrimination and oppression. The IRC directed DoD to ensure prevention
activities take these pre-military conditions and experiences into account to provide enhanced
skill development and resources for those at greatest need early in their military careers.
To support an integrated primary prevention approach across policy offices, then Acting Under
Secretary of Defense for Personnel and Readiness Matthew P. Donovan established the
Prevention Collaboration Forum (PCF) Executive Council, which includes leadership from
offices engaged in preventing self-harm and prohibited abuse and harm. DoDI 6400.09,
published by USD(P&R) in September 2020, was a collaborative effort among DoD
20
Integrated primary prevention should incorporate prevention activities at various levels of a social ecological model
(see https://www.cdc.gov/violenceprevention/about/social-ecologicalmodel.html). However, different prevention
efforts may adjust their social ecological models to account for their populations and/or the local context. For
example, a federal program may highlight the individual, organizational, and societal levels in their prevention
strategy, while a local women’s shelter may highlight the individual, family, and community levels for their
stakeholders. Social ecological models can be adapted and adjusted to fit specific prevention strategies.
21
For more information, visit https://www.cdc.gov/violenceprevention/pdf/preventingACES.pdf
14
Prevention Plan of Action
stakeholders that set forth the responsibilities and steps the Department must take to stop
harmful behaviors before they occur.
Building on the momentum of DoDI 6400.09, the Department leveraged the work of the IRC on
Sexual Assault in the Military by framing sexual assault prevention recommendations in the
context of integrated primary prevention in order to achieve benefits across the spectrum of
harmful behaviors.
To accomplish measurable and sustained reductions in harmful behaviors throughout the
military, alignment of prevention activities at all levels within an integrated primary prevention
framework is necessary. DoDI 6400.09 provides an essential first step towards integrated
primary prevention, outlining the minimum policy requirements needed across the Services to
prevent sexual assault, harassment, retaliation, suicide, domestic abuse, and child abuse. As a
critical next step, PPoA 2.0 applies current prevention science to the military environment,
clearly outlining a holistic prevention strategy that will guide prevention efforts in the years to
come.
Primary Prevention Framework applied to Integrated Primary Prevention
2.1. Prevention System - Human Resources: Leadership
Military leaders at all levels are responsible for creating and fostering a climate
grounded in mutual respect, trust, and an environment free from abuse and harm. Leaders
need to leverage their knowledge, experience, authority, and influence to set the tone for their
command climates. Leaders must have a full understanding of the prevention system and
process, and the ability to inspire support for the development, implementation, and assessment
of a comprehensive approach.
Military leaders must work closely with their prevention workforce to align their experience with
that of primary prevention science. To ensure success, leaders’ authority and operational
experience are paramount when implementing research-based prevention activities in a military
environment. Leaders must go beyond “checking the box” for primary prevention activities to
succeed. Leaders must cultivate a supportive climate by actively creating buy-in from their
subordinates, stressing that prevention is a command priority, and explaining why prevention
activities are needed in their unit. Second, leaders must proactively communicate their support
for using effective, research-based practices. The lack of visible leadership support undermines
the efficacy of proven approaches and enables the status quo.
22
Finally, the oversight capability
across the Department must hold all military leaders and the prevention workforce appropriately
accountable for adhering to the prevention process and ensuring each of the prevention system
elements is sustained over time. In effect, leader-driven prevention is crucial to generating
measurable and sustained decreases in harmful behaviors.
2.2. Prevention System - Human Resources: Prevention Workforce
Creating an organization that implements effective primary prevention requires a trained,
equipped, and resourced prevention workforce, including dedicated professional staff and
22
Gottfredson, D. C., Cook, T. D., Gardner, F. E., Gorman-Smith, D., Howe, G. W., Sandler, I. N., & Zafft, K. M.
(2015). Standards of Evidence for Efficacy, Effectiveness, and Scale-up Research in Prevention Science: Next
Generation. Prevention Science: The Official Journal of the Society for Prevention Research, 16(7), 893-926.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4579256/

15
Prevention Plan of Action
prevention enablers. The prevention workforce should also have expertise in prevention
science commensurate with their role, function, echelon, and organization. For example,
individuals in strategic and policy roles must be able to synthesize data and research and
translate the findings into policy and guidance. Individuals in organizations supporting or
overseeing individuals who implement prevention activities must be able to apply the strategic
guidance to their sphere of influence. They must also provide tools and technical assistance to
prevention professionals at the tactical level to facilitate the execution of the strategic guidance.
Individuals at the tactical level who implement prevention activities require collaboration and
facilitation skills as well as the ability to apply the strategic guidance, tools, and technical
assistance to their unique organization. In addition to these specific skills, the prevention
workforce at each level must request feedback from and provide feedback to the other levels to
assess programmatic and professional effectiveness. Ongoing, bidirectional feedback ensures
that tools, training, and technical assistance are tailored to evolving needs of diverse
organizations and their prevention workforce.
The successful implementation of effective prevention activities relies on understanding and
applying prevention research and integrating that research with leadership experience. To
ensure that implementation activities at all levels include effective, comprehensive approaches,
the Department must define and build the competencies of its workforce to use sound research
and contextualize the research with leaders’ expertise. Training curricula for the prevention
workforce must build relevant skills to identify and tailor prevention approaches to sub-
populations, such as young Service members, within the military, as applicable.
23
2.3. Prevention System - Human Resources: Military Community
The entire military community, including all Service members, military dependents, and
DoD civilian personnel, must collectively strive to create and support environments free from
abuse and harm. Members of the military community should promote DoD, military, and
Service core values through their individual actions to shape and support the norms of dignity,
respect, inclusion, and connectedness that actively deter harmful behaviors. This can include
individuals’ efforts to seek and sustain healthy and safe relationships at work and at home,
dedication to respectful and non-derogatory communication
24
with peers and significant others,
and an enduring commitment to reducing stigma and increasing support for help-seeking.
Everyone should understand how to intervene and support individuals undergoing severe stress
and/or negative life events. While individuals enter the military community with a diverse array
of backgrounds and prior experiences, attributes such as empathy need to be prioritized and
learned in order to identify individuals facing adversity and encourage them to seek help before
abuse and harm occur.
Everyone in the military community can contribute to producing the supportive climates crucial
to the success of prevention activities. Individual engagement is needed for leaders and
prevention personnel to understand the practicality and reception of different prevention
policies, programs, and practices. For example, if a program is poorly delivered, members of
the military community need to share that information with the prevention personnel evaluating
23
The term “proven prevention activity” refers to activities that have evidence of targeted behavior change or change
to one or more contributing factors, for a given population, resulting from that activity.
24
IRC recommendation 3.3b highlights the need for Service members to engage in respectful and non-derogatory
communication in virtual and cyber spaces (e.g., Tinder), as well as in person.
16
Prevention Plan of Action
the program. Proactive feedback and engagement about the military community’s needs
enables continuous evaluation, which is critical to the prevention process.
2.4. Prevention System – Collaborative Relationships
Although harmful behaviors have some unique contributing factors, they share several
risk factors (e.g., substance misuse, history of violent victimization, lack of nonviolent problem-
solving skills). These shared contributing factors can serve as the basis for collaborative
relationships. Collaborative relationships between the integrated prevention workforce and
stakeholders from other similarly invested organizations allows for greater integration of efforts.
Integrated primary prevention activities reinforce shared solutions and create opportunities for
common prevention messaging and skill development, while increasing access to those in need
via multiple sources of support. Creating complementary programming and initiatives, while
maintaining the distinct elements unique to each issue, can support an overall reduction in
harmful behaviors. Collaborative relationships require stakeholder buy-in on collective goals, a
willingness to share mutually beneficial and effective approaches, and potentially sharing
resources. Thus, each issue-specific training is reinforcing the training provided for other topic
areas and not redundant
2.5. Prevention System - Infrastructure: Data
Actionable data are critical when making prevention decisions and ensuring institutional
accountability. However, sometimes connections between a prevention activity and its long-
term outcome (e.g., lower prevalence) is unclear or too slow to observe. In such cases, leaders
and prevention personnel must leverage the substantial research that connects prevention
activities with short and intermediate outcomes (e.g., measurable success reducing a risk factor
or enhancing a protective factor). An integrated comprehensive approach focuses on doing the
greatest good for the greatest number of people; therefore, the data that are used to drive and
evaluate prevention activities must be representative of the behaviors, attitudes, and climate of
the entire organization or population, rather than specific to those who experienced harmful
behaviors or those seeking support services.
Regular assessments of the local environment are necessary so that leaders and stakeholders
can better understand “why” and “how” the prevalence of harmful incidents changes over time.
In addition, local needs assessments help each organization understand which contributing
factors leaders should prioritize for prevention. Regular assessments also demonstrate the
effectiveness of specific prevention activities in achieving their short and intermediate outcomes.
The Department must develop a dedicated and sustainable program of research to better
understand factors that contribute to harmful behaviors, methods to identify prevention activities
that mitigate those factors, and prevention metrics. Specifically, measures of effectiveness and
measures of performance for prevention planning and execution in the military environment are
needed. Moreover, data must be systematically captured, analyzed, interpreted, and shared, so
that it provides timely and accurate information to inform decisions and drive continuous
improvement at all levels
2.6. Prevention System - Infrastructure: Resources
The Department must advance and align budgets related to primary prevention to reflect
the Department’s stance toward increased prevention efforts. Depending on the unique needs
and requirements of each Service, resourcing may be required to conduct research on
the factors that contribute to harmful behaviors in unique communities, to adapt and
evaluate prevention activities prior to widespread implementation, to equip leaders with

17
Prevention Plan of Action
tools to oversee comprehensive prevention, to develop and train a prevention workforce, and to
fund implementation of local prevention activities. Resource prevention activities must be
undertaken in a way that does not diminish or degrade response capabilities.
2.7. Prevention System - Infrastructure: Policy
Establishing and strengthening prevention-related policy supports the development,
implementation, and evaluation of a comprehensive approach. Prevention policies not only
represent a portion of the prevention infrastructure and define roles, requirements, and
responsibilities; but policies are also prevention tools to achieve environmental change. Both
types of prevention policies are described here.
Prior to DoDI 6400.09, DoD policies on self-directed harm and prohibited abuse and harm
focused primarily on the response system, leaving prevention roles and requirements
unarticulated in Department policy. An effective prevention policy development identifies the
roles and responsibilities of a prevention workforce and leadership, and standards for employing
proven prevention activities as part of a comprehensive approach. Nevertheless, policies by
design are often broad and wide sweeping in their requirements. Coupling policies with
prevention expertise and leaders’ operational experience at the ground level ensures that
policies are operationalized successfully. For example, training requirements outlined in policy
may need additional specificity in terms of frequency, audience, delivery, and content.
Research-based practices and expertise of prevention experts may be leveraged by leaders to
help ensure that adaptations will not have an unintended negative impact on the program’s
effectiveness.
Prevention policies are also powerful tools to establish environments where abuse and harm are
less likely. Local policies can be altered at the installation or unit level. Policies that mitigate
situational risk factors for harmful behaviors have the potential for widespread impact within an
organization, without necessarily adding time in training.
2.8. Prevention Process - Comprehensive Approach
Consulting with subject matter experts across prevention programs will assist with
identifying prevention activities among multiple disciplines and organizations and
assist with integration of research-based activities, as appropriate. Development of a
comprehensive approach begins with the identification of key contributing individual,
interpersonal, and organizational factors. Key contributing factors then guide selection of
prevention activities that are shown to mitigate the factors in similar settings. Cohesive
alignment of selected activities allows messaging and skills from one approach to reinforce and
mutually support those of other approaches. Clearinghouses, reviews, and meta-analyses
inform sound decision-making, and provide examples of comprehensive approaches and
activities used in other communities that can serve as models for developing a comprehensive
approach in military settings.
2.9. Prevention Process - Quality Implementation
Quality implementation means effectively delivering a comprehensive approach with
fidelity in a supportive climate. Fidelity refers to delivering the approach competently as
it was originally designed. While prevention activities may be tailored or adapted to fit
the needs of a particular population, fidelity assures that the key effective ingredients of
the activity are preserved. Effective delivery means engaging the audience and key
stakeholders in a way that inspires behavior change and skill development. Process evaluation

18
Prevention Plan of Action
and research-informed strategic guidance, tools, and technical assistance facilitate quality
implementation. These functions performed by a prevention workforce at various places in an
organization ultimately support implementation of a comprehensive prevention approach in each
military setting.
Implementation of a comprehensive prevention approach must occur within a supportive
climate. In a supportive climate, leaders prioritize and value integrated prevention by ensuring
prevention activities are implemented in ways that do not produce resentment within their
subordinates or the larger military community. Prevention personnel also help produce a
supportive climate by using their specific knowledge and skills to build collaborative
relationships, guide leadership, and expertly implement prevention approaches. Service
members help sustain supportive climates by remaining open minded and willing to learn new
skills and habits when engaging in prevention activities.
25
An understanding of the degree to
which a climate supports the implementation of a comprehensive prevention approach also
enables leaders to anticipate and address barriers to success in advance of implementation.
One major factor influencing climates is the presence of negative perceptions towards
integrated primary prevention resulting from a high saturation of prevention messages and
activities in many military communities. Negative perceptions include training fatigue, low
perceived value of awareness events and related activities, and failed messaging.
Implementation of comprehensive approaches must take into account and reverse negative
impressions of primary prevention. Identification of what drives negative program associations
will allow the Department to reduce barriers that would impede positive engagement in new
proven prevention approaches. In some cases, it may be prudent to pause or stop longstanding
activities—even those that appear to be working—to address negative perceptions.
2.10. Prevention Process – Continuous Evaluation
Evaluation is an essential skill related to prevention planning and coordination.
Leadership and prevention stakeholders rely on evaluation to determine how and whether
prevention resources – money, time, and manpower – are achieving the intended outcomes.
Before a prevention activity is widely disseminated, evaluation is necessary to ensure that the
prevention approach decreases harmful behaviors or associated risk factors and is feasible for
the military environment. Prioritization of prevention activities will inform what will have the
greatest impact: activities that produce the greatest positive change should be selected over
activities that have minimal or short-lived effects. This involves engaging key stakeholders,
describing a prevention activity, defining the expected outcomes, gathering data to evaluate
progress on outcomes, using data for improvement, and disseminating lessons learned.
Continuous evaluation of a comprehensive approach is a long-term endeavor. In highly mobile
environments, continuity of effective prevention activities is important even as personnel
transition to and from units. Although some indicators of change can be realized within months
of implementing an effective and potent prevention program, detecting such change requires
systematic, valid measurement to capture subtle change over time. Evaluation that includes
assessment of multiple outcomes is necessary because comprehensive primary prevention
often includes activities that address other problem behaviors, such as harassment and alcohol
25
Scaccia, J.P., Cook, B.S., Lamont, A., Wandersman, A., Castellow, J., Katz, J., & Beidas, R.S. (2015). A practical
implementation science heuristic for organizational readiness: R = MC2. Journal of Community Psychology, 43(4):
484-501. https://pubmed.ncbi.nlm.nih.gov/26668443/

19
Prevention Plan of Action
misuse. In addition, implementing prevention approaches might first result in increases in help-
seeking behaviors and help-seeking prior to crisis. As such, regular, valid assessment of
multiple outcomes provides a clearer picture of intermediate impact.
Embedding evaluation at every level is a cornerstone of prevention. Importantly, one challenge
of the military environment is the high turnover of personnel. Leaders who embark on a mission
to support and sustain prevention activities may not witness the results or outcomes of their
programs. Prevention personnel must manage expectations of individuals or institutions
desiring rapid results. For example, it can take over ten years to fully evaluate the effects of a
prevention program. Nonetheless, slow, steady progress should not dishearten leaders or halt
evaluation efforts. Instilling evaluation as a normal part of the prevention process requires an
assessment of the current state of evaluation and the prevention system elements necessary for
evaluation. The Department must take systematic steps to evolve toward more rigorous
evaluation for untested prevention activities. This process likely entails prioritizing activities that
are ready for evaluation as well as evaluating activities that are already widely disseminated but
not yet tested.
DoD Integrated Primary Prevention Goals
Establishing an optimized organization that supports and sustains the development,
implementation, and evaluation of a comprehensive primary prevention approach is a long-term
endeavor. Between 2019 and 2022, the Department took some steps towards this goal by
completing six of twenty-two objectives from the PPoA 1.0. The original PPoA pushed the
Department and the Services to take key steps towards building a robust prevention system and
engaging in prevention activities using a public health approach. Key milestones achieved to
meet PPoA objectives include: 1) development of metrics and thorough self-assessment across
DoD to identify prevention strengths and gaps, 2) developing and fielding of a public health
curriculum designed for prevention professionals in the military, and 3) the release of a research
agenda that summarizes the DoD’s highest priority research topics and methods.
On September 22, 2021, the Secretary of Defense approved the implementation of the
recommendations laid forth in the IRC Report, wherever possible. An “Implementation
Roadmap” that outlines key milestones and timelines was developed by the Department to
guide implementation efforts of the recommendations as approved by the Secretary of Defense.
Deadlines for implementation are nested into four tiers: Tier 1 must be completed by FY27, Tier
2 and Tier 3 must be completed by FY28, and Tier 4 must be completed by FY30.
26
The Department is implementing the following approved recommendations in the context of
integrated primary prevention. Implementation will be tracked through a single reporting
process.
26
Tier 1 implements the approved recommendations that build the Department’s basic foundation and infrastructure
for sexual assault accountability, prevention, and response programs with estimated completion FY 2027. Tier 2
implementation is dependent on the execution of a Tier 1 actions and builds directly on that Tier 1 infrastructure to
apply strategies (e.g., training, education) with estimated completion in FY 2028. Tier 3 recommendations are either
chronologically or practically dependent on the execution of a Tier 2 action, and would expand programs and
practices within the DoD, or would endure throughout the implementation process. Lastly, Tier 4 actions are either
chronologically or practically dependent on the execution of a Tier 3 action or would expand programs and practices
outside of the DoD purview with estimated completion in FY 2030. DoD Actions and Implementation to Address
Sexual Assault and Sexual Harassment in the Military (defense.gov)

20
Prevention Plan of Action
IRC Recommendation 2.1 a:
USD(P&R) should define the competencies leaders must
have to oversee prevention. (Tier 1, Estimated completion:
FY 2027)
IRC Recommendation 2.1 b:
The Services and the National Guard Bureau (NGB) should
develop and hold leaders appropriately accountable for
prevention. (Tier 3, Estimated completion: FY 2028)
IRC Recommendation 2.1 c:
The Services and the NGB should equip all leaders to
develop and deliver informed prevention messages in formal
and informal settings. (Tier 2, Estimated completion: FY
2028)
IRC Recommendation 2.2 a:
USD(P&R) should develop a model for a dedicated and
capable prevention workforce. (Tier 1, Estimated completion:
FY 2027)
IRC Recommendation 2.2 b:
USD(P&R) should develop a professional credential for the
prevention workforce. (Tier 1, Estimated completion: FY
2027)
IRC Recommendation 2.2 c:
The Services should determine the optimum full-time
prevention workforce, and equip all echelons of active duty,
reserve, and guard organizations. (Tier 1, Estimated
completion: FY 2027)
IRC Recommendation 2.3 a:
The Services and the NGB should resource and implement
prevention strategies at organizational and community levels.
(Tier 3, Estimated completion: FY 2028)
IRC Recommendation 2.4:
Modernize prevention education and skill-building to reflect
today's generation of Service members. (Tier 2, Estimated
completion: FY 2028)
IRC Recommendation 2.5 a:
The Services and the NGB should institute a pilot program to
link Service members with resources and support. (Tier 1,
Estimated completion: FY 2027)
IRC Recommendation 2.5 b:
The Services and the NGB should employ virtual-platforms to
provide support to all Service members. (Tier 1, Estimated
completion: FY 2027)
IRC Recommendation 2.6 b:
USD(P&R), the Services, and the NGB should continually
review and update all policies that unnecessarily restrict data
collection on important populations of Service members.
(Tier 1, Estimated completion: FY 2027)

21
Prevention Plan of Action
IRC Recommendation 2.7b:
USD(P&R) should submit a legislative proposal providing
authorization and funding for the NGB to conduct recurring
National Guard unit inspections and staff assistance visits for
prevention oversight and assistance. (Tier 1, Estimated
completion: FY 2027)
IRC Recommendation 2.8:
USD(P&R) should update the Department's prevention
strategy, including the DoD Prevention Plan of Action, to
incorporate approved IRC recommendations. (Tier 4,
Estimated completion: FY 2030)
IRC Recommendation 3.2:
USD(P&R) should direct the Services to educate the force
about sexual harassment and sexual assault within the
context of the Services’ core values.
27
(Tier 2, Estimated
completion: FY 2028)
IRC Recommendation 3.7 a:
USD(P&R) should develop a standardized "pulse survey" tool
that would enable unit-level commanders to collect real-time
climate data on sexual harassment and sexual assault from
Service members in their units between required
administrations of the Defense Organizational Climate
Survey (DEOCS). (Tier 1, Estimated completion: FY 2027)
IRC Recommendation 3.7 b:
The Secretary of Defense should direct the Services to
develop a formal system to share climate survey data at the
unit level and initiate and evaluate corrective action plans.
(Tier 1, Estimated completion: FY 2027)
IRC Recommendation 3.7 c:
USD(P&R) should accelerate efforts to develop a validated
"Climate Benchmark" to measure healthy and unhealthy
climate at the unit level. (Tier 1, Estimated completion: FY
2027)
IRC Recommendation 3.6:
Building a climate for the reduction of sexual harassment and
sexual assault as a fundamental leader development
requirement.
28
(Tier 2, Estimated completion: FY 2028)
PPOA Objective 4.9.4:
Address evaluation gaps and develop, implement, and
institutionalize an evaluation process by which prevention
programs and activities are evaluated and results are
disseminated to support continuous quality improvement.
(Estimated completion: FY 2028).
27
For the purposes of this PPoA, Recommendation 3.2 will be applied across harmful behaviors.
28
For the purposes of this PPoA, Recommendation 3.6 will be applied across harmful behaviors.

22
Prevention Plan of Action
Sec 549A FY22 NDAA:
Beginning on October 1, 2022, and annually on the first day
of each fiscal year thereafter, the Secretary of Defense shall
publish a Department of Defense research agenda for that
fiscal year, focused on the primary prevention of
interpersonal and self-directed violence, including sexual
assault, sexual harassment, domestic violence, child abuse
and maltreatment, problematic juvenile sexual behavior,
suicide, workplace violence, and substance misuse.
29
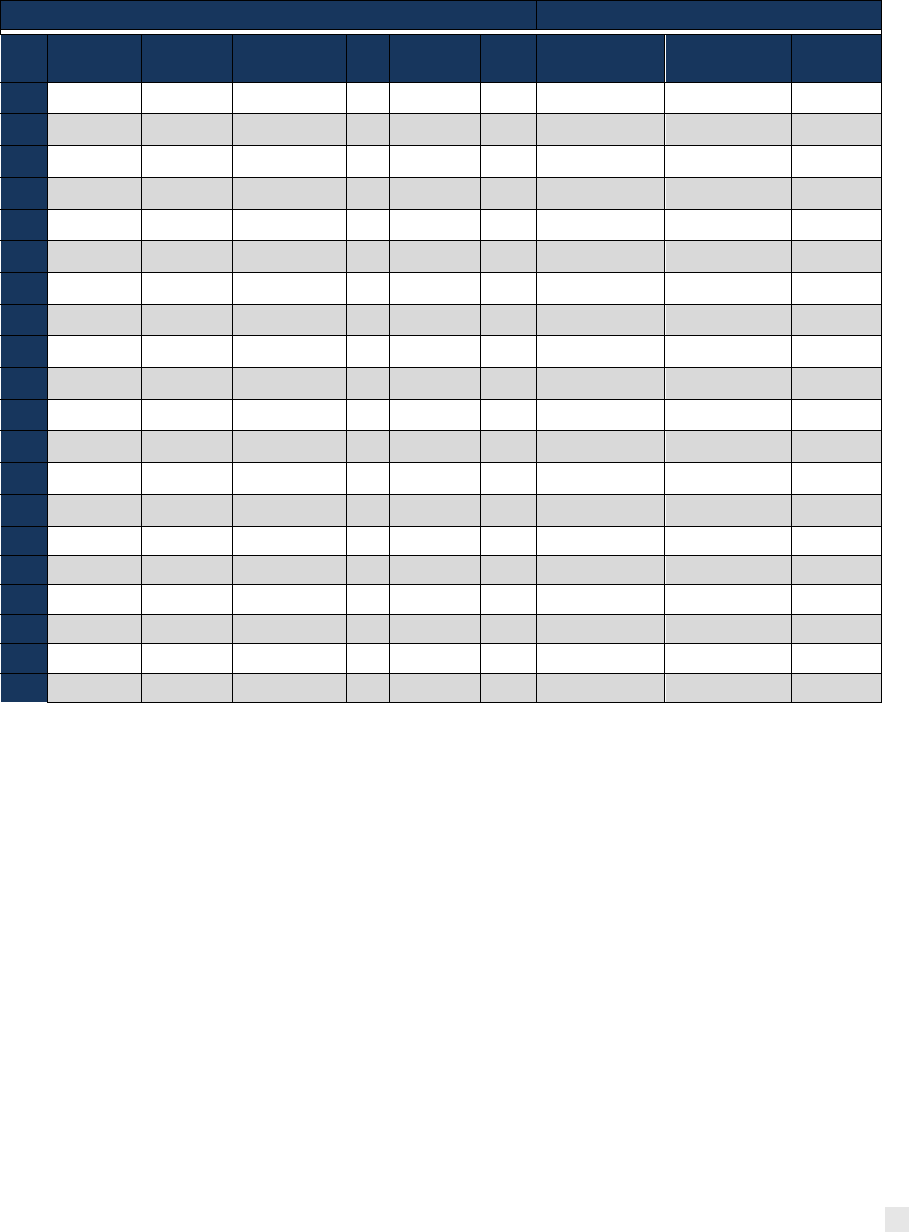
In many cases, the Department’s implementation guidance regarding the approved IRC
recommendations
30
will require coordination. Table 1 provides an overview of the interplay of
the approved recommendations and the elements identified to ensure successful
implementation.
29
United States National Defense Authorization Act for Fiscal Year 2022: Report of the Committee on Armed
Services, House of Representatives. Washington: U.S. Government Publishing Office. Section 549A.
30
Under Secretary of Defense Personnel and Readiness Memorandum, “Guidance for implementing Tier 1
Recommendations of the Independent Review Commission on Sexual Assault in the Military,” October 13, 2021.
Under Secretary of Defense Personnel and Readiness Memorandum, “Guidance for implementing Tier 2
Recommendations of the Independent Review Commission on Sexual Assault in the Military,” November 12, 2021.
Under Secretary of Defense Personnel and Readiness Memorandum, “Guidance for implementing Tier 3 and 4
Measures Related to Recommendations of the Independent Review Commission on Sexual Assault in the Military,”
December 15, 2021.
23
Prevention Plan of Action
Table 1. Map of PPoA 2.0 Elements and IRC Recommendations
PREVENTION SYSTEM
PREVENTION PROCESS
Rec
Leadership
Prevention
Workforce
Collaborative
Relationships
Data
Resources
Policy
Comprehensive
Approach
Implementation
Evaluation
2.1a
X
X
2.1b
X
X
X
2.1c
X
X
X
2.2a
X
X
2.2b
X
X
2.2c
X
X
2.3a
X
X
X
X
X
X
X
X
2.4
X
X
X
X
2.5a
X
X
X
X
2.5b
X
2.6d
X
X
X
X
2.7b
X
X
X
X
X
2.8
X
X
X
X
3.2
X
X
X
X
3.6
X
X
X
3.7a
X
X
X
X
X
X
X
3.7b
X
X
X
X
X
X
X
3.7c
X
X
X
X
X
X
4.9.4
X
549A
X
Prevention Oversight
The oversight of the integrated primary prevention-related IRC recommendations will be
conducted by the Office of the Secretary of Defense for Personnel and Readiness. The
Prevention Collaboration Forum and the Violence Prevention Cell may provide technical
assistance to the Military Departments, Services, and National Guard Bureau to monitor and
ensure standardization, where appropriate, of implementation.

24
Prevention Plan of Action
Appendix A
Glossary
Child Abuse: Defined in DoDI 6400.01.
Collaboration: Exchanging information, altering activities, sharing resources, and enhancing
each other’s capacity for mutual benefit and a common purpose in accordance with law and
DoD regulations.
Credential: A process for verifying preparation, additional training, and/or prior work
experiences of prevention human resources by the awarding of either a certificate or
certification.
Continuous Evaluation: Routinely analyzing information and data to determine if prevention
activities are changing the factors they were designed to address. This includes evaluation of
activities and program outputs as well as evaluation of program outcomes.
Data-driven Actions: Defined in DoDI 6400.09.
Discriminatory Harassment: Defined in DoDI 1020.03.
Domestic Abuse: Defined in DoDI 6400.06.
Evaluation: The use of systematic methods to collect, analyze and use information to inform
implementation of a policy, program, practice, or processes.
Evidence-Based: Effective policies, programs, practices, or processes that are evidence-
based are found to be effective based on research evidence, reflecting significant expertise and
investment.
Fidelity: Refers to delivering the approach competently and as it was originally designed.
Harassment (Service Member): Defined in DoDI 1020.03.
Harassment (Civilian): Defined in DoDI 1020.04.
Harmful Behaviors: Self-directed harm and prohibited abuse and harm, including sexual
assault, harassment, retaliation, suicide, domestic abuse, and child abuse.
High Risk Groups or Subpopulations: Defined in DoDI 6400.09.
Integrated Primary Prevention: Defined in DoDI 6400.09.
Military Community: Defined in DoDI 6400.09.
Military Leaders: Defined in DoDI 6400.09.
Outcome Evaluation: A systematic process for collecting information to determine the degree
to which, if at all, a policy, program, or practice is affecting the intended target population(s) and
whether or not program improvements are needed to achieve intended outcomes.
Practice: Discrete behavior or action contributing to prevention.
Prevalence: Defined in DoDI 6400.09.
Prevention Activities: Defined in DoDI 6400.09.

25
Prevention Plan of Action
Prevention Workforce: A subset of prevention personnel whose official duties (to include
collateral and additional duties) involve prevention of self-directed harm and prohibited abusive
or harmful acts and who attain and sustain prevention-specific knowledge and skills (e.g.,
chaplains, suicide prevention program managers, command climate specialists).
Primary Prevention: Defined in DoDI 6400.09.
Prevention Process: Empirically validated procedures that promote effective planning,
implementation, and evaluation of prevention activities (Error! Reference source not found.).
Program: Curriculum or manualized set of activities and information intended for cognitive
learning and skill development.
Protective Factors: Defined in DoDI 6400.09.
Public Health Surveillance Methods: The ongoing, systematic collection, analysis, and
interpretation of health-related data essential to planning, implementation, and evaluation of
public health practice.
Research-based Prevention Activities: Defined in DoDI 6400.09.
Risk Factors: Defined in DoDI 6400.09.
Sexual Assault: Defined in DoDI 6495.02, Volume 1.
Self-directed harm: Defined in DoDI 6400.09.
Selected Primary Prevention: Takes place BEFORE violence initially occurs. It involves
programs and strategies designed to reduce the factors that put people at risk for experiencing
violence. Or, they encourage the factors that protect or buffer people from violence. Prevention
efforts focused on those individuals or groups that show one or more risk factors for violence.
Sexual Harassment: Defined in DoDI 1020.03.
Sexual Minority: A group whose sexual identity, orientation or practices differ from the majority
of the surrounding society. Primarily used to refer to lesbian, gay, bisexual, or non-heterosexual
individuals.
Social Determinants of Health: Conditions in the environments in which people are born, live,
learn, work, play, and worship that affect a wide range of health, functioning, and quality-of-life
outcomes and risks.
Social Ecological Model: The social ecological model understands health and well-being to
be affected by the interaction between the individual, interpersonal, and organizational factors.
Stalking: Defined in DoDI 1020.03.
Suicide: Defined in DoDI 6490.16.
Toxic leadership: An individual’s perception that their leader has a disregard for subordinate
input, defiance of logic or predictability, and self-promoting tendencies. “Toxic Leadership”
behavior includes demeaning/marginalizing, degrading, coercion, deception, and angry/acts of
aggression.
Universal Primary Prevention: Primary prevention activities are directed at the general
population and attempt to stop maltreatment before it occurs. All members of the community
have access to and may benefit from these services. Primary prevention activities with a

26
Prevention Plan of Action
universal focus seek to raise the awareness of the general public, service providers, and
decision-makers about the scope and problems.
